What Causes an Acoustic Neuroma?
Genetic factors play a large role in the formation of acoustic neuromas. A mutation in a tumor-suppressor gene on the long arm of chromosome 22 is found in acoustic neuromas, and is responsible for their growth. In most cases this mutation is not inherited, rather it is a spontaneous mutation effecting the growth of schwann cells on the eighth nerve. Some patients have an inherited mutation effecting chromosome 22 resulting in a genetic disorder known as Neurofibromatosis type II (NF-2). The mutation causing NF-2 is autosomal dominant and may be passed to offspring. The hallmark of NF-2 is the presence of bilateral acoustic neuromas, unlike the spontaneous mutation which results in unilateral acoustic neuroma formation. Patients with NF-2 are also at increased risk of developing certain tumors of the brain and spinal cord.
How Is an Acoustic Neuroma Diagnosed?
Patients commonly present to physicians with complaints of hearing loss, ringing in the ears (tinnitus) and dizziness. Often an MRI of the brain is obtained to evaluate these complaints, revealing an acoustic neuroma. Sometimes the patient is sent for a hearing test to evaluate symptoms of hearing loss. The hearing test may show a pattern of hearing loss characteristic of acoustic neuromas. Once diagnosed with an acoustic neuroma, patients are sent to a neurosurgeon to discuss treatment.
How is an acoustic neuroma treated?
In cases where the tumor is very small with out any associated symptoms, the acoustic neuroma may be observed. In cases where the tumor is large and the symptoms more severe, surgical treatment is often advocated. When surgery is considered several approaches may be used. The size of the tumor and the patient’s pre-operative hearing function are often taken into consideration when planning the operative approach.
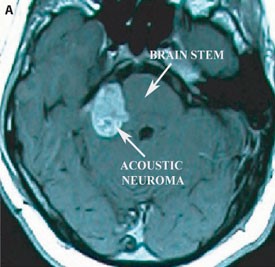
A) Pre-operative axial T1 MRI with contrast demonstrating a large acoustic neuroma compressing the brainstem
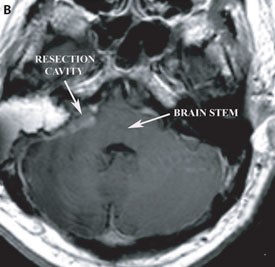
B) Post-operative axial T1 MRI with contrast demonstrating the surgical resection cavity and resolution of brain stem compression