What Causes Cerebral Aneurysms?
The causes of cerebral aneurysms are not completely understood. Patients with hypertention or who smoke are at an increased risk of developing aneurysms. There are also certain genetic conditions that predispose a patient to developing an aneurysm, such as: polycystic kidney disease, fibromuscular displasia, and a variety of connective tissue disorders. Patients with multiple family members who have aneurysms are also at increased risk of having an aneurysm themselves. Some aneurysms, termed mycotic aneurysms, can even arise from an infectious process.
How Are Cerebral Aneurysms Discovered?
Some aneurysms are found by accident. For example, an unruptured aneurysm can be detected when a patient receives an MRI of the brain to evaluate a minor headache or dizziness. Often these aneurysms are incidental findings, and have no relation to the patient’s symptoms.
Sometimes aneurysms are discovered through the routine screening of high risk patients. Other times aneurysms are discovered when they rupture. When an aneurysm ruptures a patient frequently experiences a sudden onset excruciating headache, sometimes accompanied by lethargy and possible loss of consciousness.
How Are Cerebral Aneurysms Treated?
The treatment of cerebral aneurysms is complex and it is critical that the patient is evaluated by both a neurointerventionalist and a neurosurgeon to ensure that they are properly counseled on their options before a treatment plan is formulated. There are three options available for treating aneurysms: observation and medical management, surgical repair of clipping, and neurointerventional therapy
Observation and medical management is only an option for unruptured aneurysms. This form of treatment involves smoking cessation, blood pressure management, and periodic radiographic imaging of the aneurysm to monitor the size and possible growth of the aneurysm.
Surgical repair of cerebral aneurysms, while invasive, is an important option for the treatment of aneurysms. Recent advances, such as use of the operating microscope, the increasing mechanical sophistication of the aneurysm clips and improved techniques for neuroprotection have helped improve the safety and efficacy of the surgical treatment of cerebral aneurysms.
Neurointerventional treatment of cerebral aneurysms has been available since the 1970s, and has rapidly evolved into an effective minimally invasive treatment modality. Using x-ray guidance, a neurointerventionalist advances a catheter from an artery in the groin to the artery in the brain where the aneurysm is located. Then, a variety of detachable platinum “coils” are used to fill the aneurysm. Using this technique, durable and complete occlusion of the aneurysm with markedly reduced risk of bleeding, similar to traditional surgery, can be achieved in most patients. In many patients, this new method of minimally invasive treatment is often a safe and effective alternative to traditional surgery. Not all patients are eligible for this type of minimally invasive treatment and traditional surgical clipping remains an important and effective option in many patients.
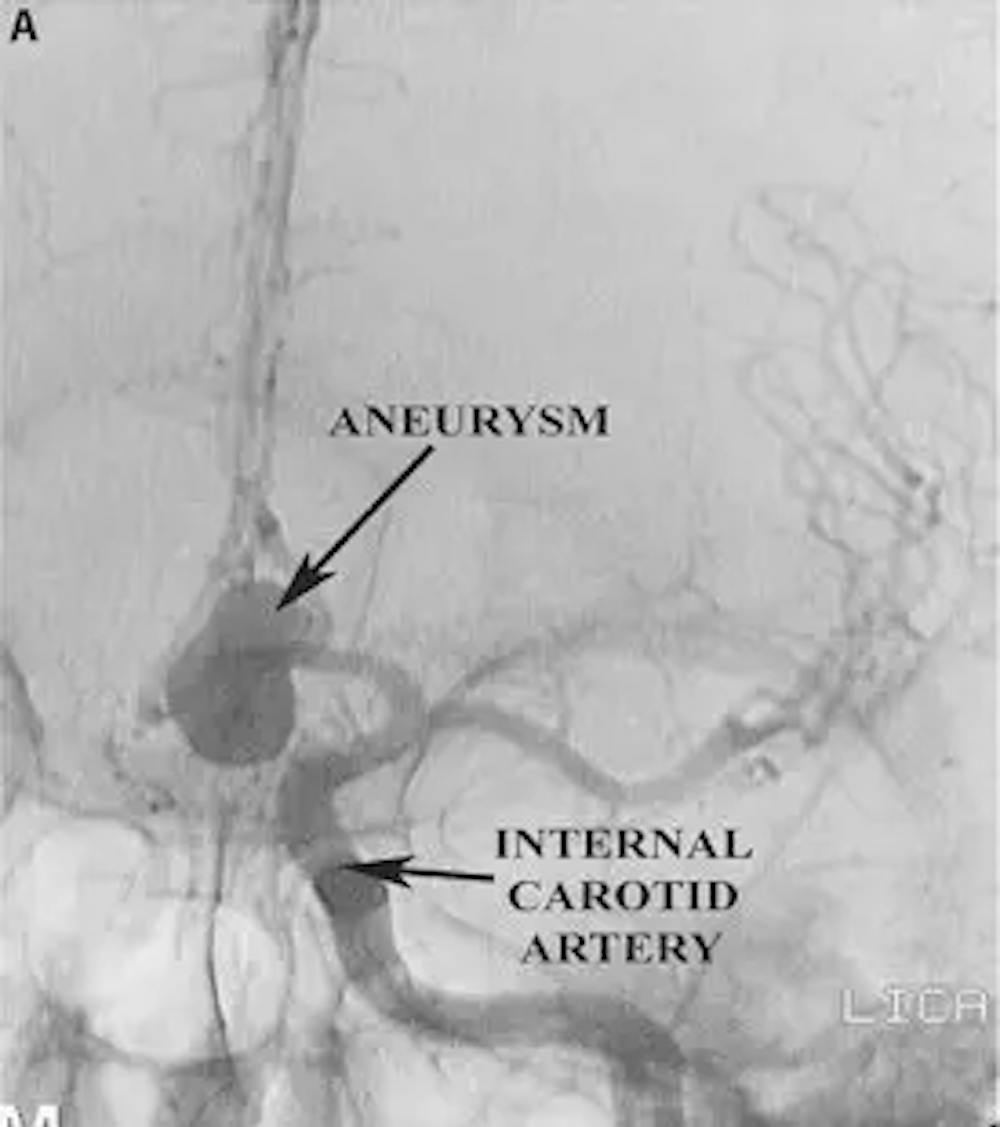
A) Pre-operative AP angiogram demonstrating a large anterior communicating artery aneurysm
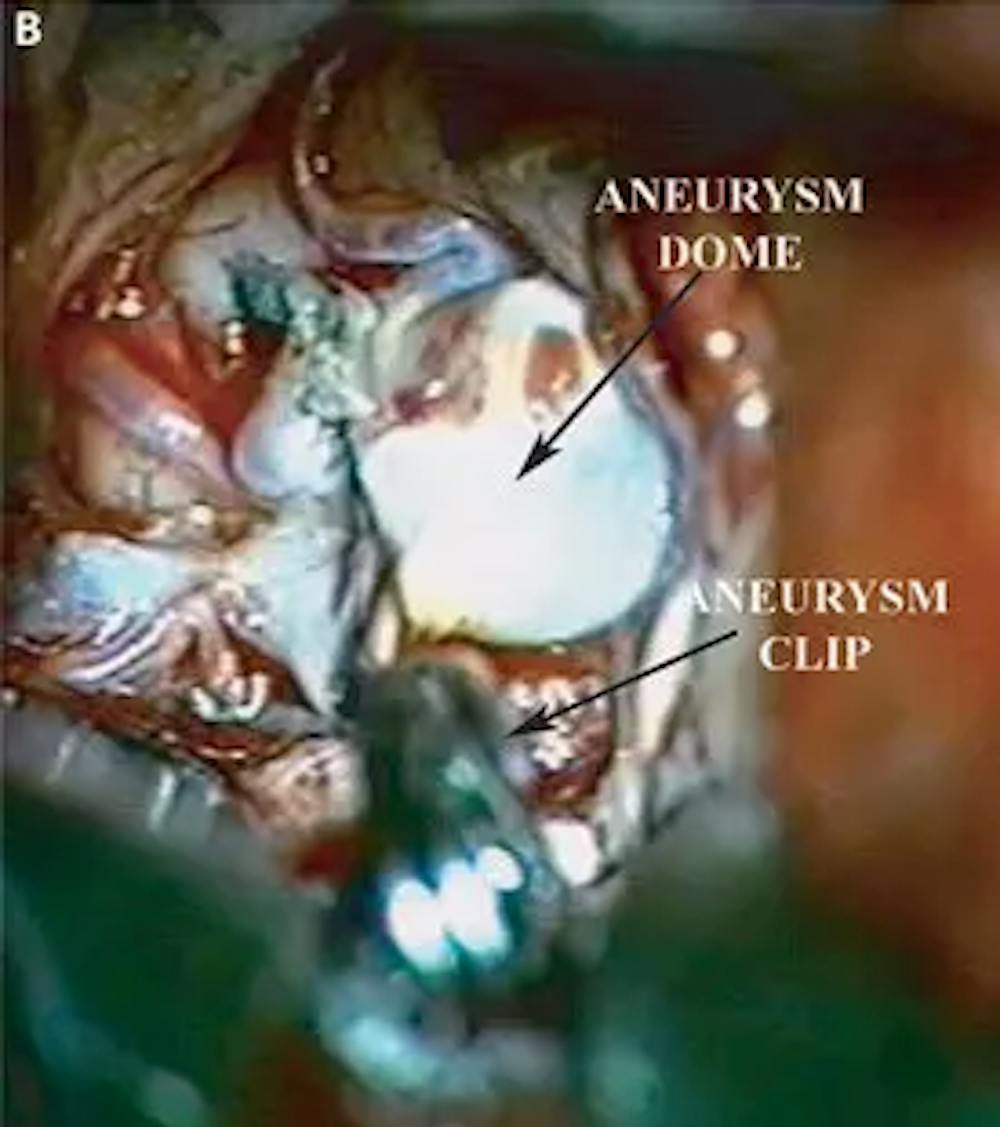
B) Intra-operative photo demonstrating clip placement on the neck of the aneurysm

C) Post-operative AP angiogram demonstrating clipping of anterior communicating artery aneurysm